Tuesday, August 31, 2004
Had a good time in Martha's Vineyard for the family wedding. It was a very nice place with excellent seafood. On a bus tour we took the driver name dropped during the whole trip, telling us where Michael J. Fox's house was, where the Clinton's had bought land a week ago, where John Belushi is buried, ect, ect,ect....
The Vinyard seems to be a safe place as the police seemed bored and the bed and breakfast where I was staying kept the door unlocked. However I heard that O.J. Simpson had been seen earlier that week, so I was afraid the Real Killers were nearby. Below are pictures of the clay cliffs of Aquinnah.



My wedding attire caught alot of glances as well. It was like no one had seen a seeersucker suit before. I took great delight in telling people that everyone in the south dressed like that.
|
Lifted from Overlawyered, the story of a $366 million verdict against the medical director of a hospital cath lab, the head of the cardiology section, and the chief of medicine surrounding a suspension of Dr. Poliner's cardiac cath privileges. Apparently there were some concerns over Dr. Poliner's work expressed by nursing staff. There was also an allegation of wrong site intervention. A peer review committee suspended his privileges, which were re-instated after outside review. As Mr Frank succinctly puts it:
So far, so good, right? After all, we're told by the plaintiffs' bar that the medical malpractice crisis would go away magically if the medical profession would just police its own, and that's exactly what happened here. Can you imagine what a trial lawyer would do with the peer review committee's conclusions if the hospital did nothing and had been sued for Poliner's work afterwards?Dr. Poliner then goes on to sue the physicians involved.
The suit alleges that doctors who were competing with Dr. Poliner for patients accused him of poor patient care, and that Dr. Knochel (chairman of internal medicine) and Presbyterian relied on the competitors rather than independent reviews to conclude that Dr. Poliner's right to perform catheterizations and echocardiograms should be suspended.The suits against the peer-review committee were dismissed, but the suits against the others was allowed to proceed, with the results described above. The hospital plans an appeal. Now other than the punishment of a hospital trying to maintain quality, two other issues come out of this. First:
In May 1998, Dr. Knochel forced Dr. Poliner to quit doing catheterizations while the hospital reviewed his work.
A month later, a peer review committee of doctors, most of whom competed for patients with Dr. Poliner, summarily suspended his "cath" and "echo" privileges at Presbyterian. In November 1998, the hospital's medical board voted to restore Dr. Poliner's privileges after a number of nationally recognized cardiologists in a hearing stoutly defended the quality of Dr. Poliner's work. However, the medical board also upheld Dr. Knochel's earlier decision to suspend Dr. Poliner's privileges.
"From time to time, hospitals and members of the medical staff leadership must make decisions relating to patient care and safety, and these decisions sometimes affect an individual doctor's privileges at that hospital," the hospital said in a statement.That is, the chairs of departments and other physician leaders who are often the initial contacts in such issues may be exposed to liability in carrying out their responsibilities under hospital bylaws. Given the difficulty in finding physicians to fill those roles, this will only further serve to discourage physicians from taking leadership positions on their medical staffs.
Secondly, and here is where IMHO the hospital dropped the ball, was the lack of outside review. Outside of a large metropolitan area, such as Atlanta for example, it is difficult to find members of a peer-review committee who are not in competition with or refer patients to, a physician who may be under investigation. Hospital medical staffs are some of the most ruthless political operations today, some make Tammany Hall look like amateur hour. These situations almost always require outside review to maintain impartiality. The problem then becomes finding a reviewer to do this, as they may be liable in a suit as well. I have told the story before of a physician who threatens to sue his own specialty organization when they agree to review his situation. Needless to say they beat a hasty retreat. So outside review may not be possible.
The way to fix this? Expand the peer review protection to members of the medical staff engaging in good-faith quality assurance and to outside reviewers.
Cross-posted at Galen's log
|
Monday, August 30, 2004
From American Medical News: Ballot battle: Two professions square off over attorney fees and quality of care.
Doctors and lawyers in Florida have taken the tort reform fight to a new level -- dueling ballot initiatives.The amendment would propose that attorneys would be limited to 30% of any award up to $250,00 and 10 percent of any monies above that. According to the article, the expenses incurred by the attorney would not be subject to the cap. As you can imagine, the trial bar is crying:
On Nov. 2, Florida citizens will vote "yes" or "no" on three proposed constitutional amendments that address medical liability issues. Early polling shows that all of them are likely to pass.
The ballot box battle comes a little more than a year after the Florida Legislature passed a $500,000 noneconomic damages cap that doctors say won't prevent premium hikes that are forcing them to leave the state, retire early or forgo high-risk procedures.
To solve the problem, doctors are proposing a constitutional change that would limit the amount that trial lawyers could collect in medical malpractice lawsuits so that injured patients get a bigger chunk of awards.
Trial lawyers are proposing two constitutional amendments. The first -- commonly referred to as the "three-strikes" rule -- calls for stripping doctors of their medical licenses if they have three medical malpractice judgments against them. The second amendment would let patients see medical records and reports connected with "adverse" incidents, including documents generated during peer-review procedures.
The doctors' proposed amendment would reduce accountability for health care negligence and incompetence, said Patti O'Regan, a nurse practitioner and a board of governors member for Floridians for Patient Protection, an advocacy group formed to put the trial lawyers' amendments on the ballot.Let's look at the numbers, shall we. Given the average payout in 2002 was $3.9 million in the U.S. and MAG Mutual had an average payout of $4.6 million that would allow the attorney to collect, on top of expenses, $440,000 on the U.S. average and $510,000 on the MAG average. Not exactly chump change.
If lawyers' share of awards was limited, patients would be forced to pay lawyers by their hourly fees, she said. Patients who don't have enough money to pay those charges wouldn't have access to the courts.
"Only the wealthiest Americans, such as doctors, will be able to find and pay for attorneys to take their cases," O'Regan said. "The safety net of contingency fee arrangements is the only access middle-class and poor Americans will have to the court system."
The physicians' amendment "would act as a total ban on medical malpractice cases because you wouldn't be able to find a lawyer to take a case," said trial lawyer Susser. "It takes so much money to fight these people."
On to round two:
Under Amendment 8, physicians would lose their licenses if they had three strikes against them, including final court judgments, final administrative agency decisions or binding arbitration. Lawyers say patients would be safer because doctors with repeated judgments against them wouldn't be allowed to treat patients....The proposed amendment would do what the Florida Board of Medicine has been too afraid to do, O'Regan said. "It gets rid of doctors who refuse to learn from their mistakes and improve their service to patients," she saidIf you look here you certainly see that the authorities in Florida have been quite busy in laying down the law on a wide variety of medical professionals. If this passes then there will be not only financial pressure to settle, but also to avoid getting a strike.
But doctors counter that the amendment would not accomplish that goal. Instead, they say, it would exacerbate the existing medical liability problem. Fearing that they could lose at trial even though they have a solid defense, doctors would be more likely to settle malpractice or negligence cases instead of taking their chances before juries, physicians say.
The last amendment would serve a severe blow to patient privacy by allowing access to the records of "adverse events":
Under Amendment 7, patients would be able to review medical records associated with adverse medical incidents involving facilities and health professionals. Patients' identities would not be disclosed.This wouldn't help peer review at all. One reason peer review doesn't work is the medical staff/physician part of it will recommend suspension or removal from a medical staff but the hospital administration will get gun shy when, surprise, the subject of the review threatens to file suit.
A more open system, trial lawyers argue, would prevent errors from being swept under the rug and would help patients make more educated choices when picking physicians.
"Peer review isn't working," O'Regan said.
All of the amendments seem likely to pass:
Limiting attorney fees 74%If any of the last two pass, it will do far more damage than the first amendment can ever help to mend. So the people of Florida will have their vote, and the physicians may cast theirs, with their feet, and leave Florida.
Taking away a medical license after
three judgments against a physician 78%
Allowing patients to see records
tied to adverse incidents 75%
Cross-posted at Galen's Log |
What was it that Groucho Marx said?
"I don't care to belong to a club that accepts people like me as members"Well I am honored to be invited to join Galen's Log as a guest author. I am eager to be a member of the medical blogosphere's latest troikia. It's gonna be a blast...
Cross-posted at Galen's Log |
Wednesday, August 25, 2004
Taking a week off to go to a family wedding in New England. It will be good to get away for a while as I am getting a little bitter with work right now.
As a parting thought I leave you this. An older physician brought this up the other day during a discussion about liability premiums and declining reimbursement. It is a good, simple expression about the frustration many physicians feel:
Why am I worth so little when I do my job right, and worth so much when I make a mistake?
Good-bye until next week.
|
Tuesday, August 24, 2004
A commenter to this post asked:
If what Mr. Rehberg et al says about the hospital's practices is true, the motivation in coming forward is irrelevant. Wouldn't the practices be illegal?That is the crux of the whole matter, were the practices illegal? Given the widely accepted interpretation of Medicare regulations before the February 2004 memo, their actions were, IMO, within the law. There are no clear requirements for not-for-profit organizations in relation to charity care.
As there may be some confusion, allow me to explain. The Acme Surgical Company has a list of what we consider our "usual and customary fees". These date back tp the time before managed care when private insurance would pay the charges within reason. We have contracts with managed care and insurance companies which define a reimbursement for a service which have little or no relation to those "usual and customary fees". We cannot, under the contract, "balance bill' the patient for the difference. In exchange for that "discount", if you will, we are given access to the "insured lives" of that company as well as being reimbursed directly by the company rather than the check going to the patient. "Medicare assignment" works the same way. We cannot have "usual and customary fees" below that of Medicare. From the memo:
As noted in the preamble to the proposed regulations, the exclusion provision does not require a hospital to charge everyone the same price; nor does it require a hospital to offer Medicare or Medicaid its "best price." However, hospitals cannot routinely charge Medicare or Medicaid substantially more than they usually charge others.So given a vague regulation relating the discounting of care the hospital is going to act in a way to avoid the scrutiny of a Medicare audit. That means that as far as charges go, Medicare serves a floor, not a ceiling.
|
From the Atlanta Journal-Constitution:Medicaid overhaul pushed
The state plans to move 1 million low-income Georgians on Medicaid into HMO-like organizations - a cost-cutting tactic representing one of the biggest changes in the government program's history.Perhaps my memory fails me. Wasn't this tried with Medicare in the not-so-distant past, with a poor showing? Didn't many insurers get out of the Medicare HMO business because they lost a great deal of money? What makes Governor Perdue think it will work for the Medicaid population? Do tell. Oh, and it has been tried before:
The plan, unveiled Monday, is being pushed by Gov. Sonny Perdue as a response to spending increases of 10 percent to 12 percent a year in Georgia Medicaid.
Georgia had a voluntary HMO program in the 1990s for Medicaid, but the effort proved unsuccessful at attracting a large number of people willing to enroll.The discussion over the breakfast table this morning found little support for the proposal. With only one orthopedist and half of the OB/GYN's accepting Medicaid nowadays in River City the chances of this being a success is low.
|
Had planned a lengthy rant today on an issue of import, but silly day job reared its' ugly head. Anyway, a brief discussion of how the use of thoracic CT is expanding.
70-ish restrained passenger struck on their side of vehicle. +LOC. GCS 15 0n arrival. Main complaint is of back pain. Physical exam unrevealing. Initial CXR:
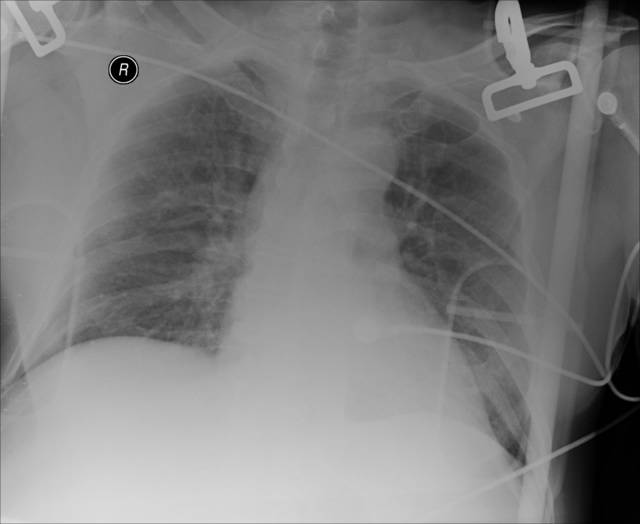
Not much to see. But as my use of FAST has reduced the number of abdominal CTs I order on trauma patients, the number of chest CT's I order has increased. From the May 2002 Journal of Trauma: Incidence and Characteristics of Motor Vehicle Collision-Related Blunt Thoracic Aortic Injury According to Age.
Abstract:But submitting Grandma and Grandpa to thoracic angiograms is not a benign course of action. The use of thoracic CT has made the diagnosis of the injuries simpler.
Background : Motor vehicle collision-related blunt thoracic aorta injury (BAI) is rare and highly lethal. Vascular disease as related to advancing age potentially subjects older adults to increased risk of BAI; the mechanisms associated with such injuries may be different as compared with younger adults. The goal of the present study is to test this hypothesis using population-based data.
Methods : The 1995 to 1999 National Automotive Sampling System data files were used. The National Automotive Sampling System is a national probability sample of passenger vehicles involved in police-reported tow-away crashes. BAI was defined according to the Abbreviated Injury Scale codes. Among those with BAI, information on occupant (age, seating position, restraint use), collision (collision type, delta-V, vehicle intrusion), and outcome characteristics were obtained and compared according to age.
Results : The overall incidence of BAI was 6.8 per 10,000 occupants and there was a steady increase in the BAI rate for advancing decades of life. The proportion of occupants with BAI who die at the scene of the collision is relatively consistent across all age groups (~85%). Among those who survive to receive medical care, ultimate survival is lowest among those aged 60 and older. Near-side collisions were responsible for more BAI among older adults than other age groups (50% vs. 20.6%, p <= 0.05). Older adults sustained BAI in collisions with lower delta-V values compared with younger persons (p <= 0.05). Conclusion : Older adults have the highest rate of motor vehicle collision-related BAI, and their injuries tend to occur in less severe collisions. A high level of suspicion for BAI among older adults should not be reserved for high-energy collisions only.
I did perform a FAST exam, and I could not get good visualization of the splenorenal space very well. Off to CT. Solid organs look O.K., but look what we found:
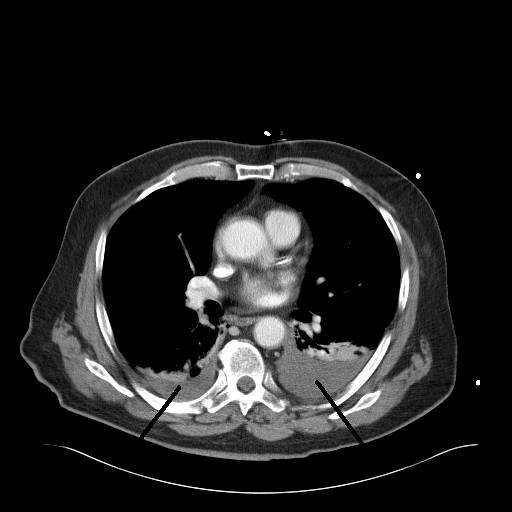
There is about 500cc of blood on the left and 75cc on the right. Here is the dual exhaust film:
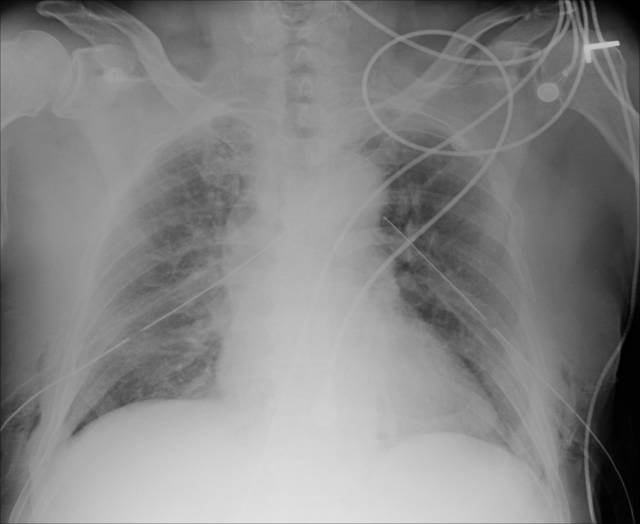
While the hemothorax was not hemodynamicaly significant, blood left in the chest can lead to empyema, fibrothorax, and entrapment of a lobe. These conditions can lead to a thoracotomy and decortication. Not fun.
See this post from Shazam for more CT scanning adventures.
|
Saturday, August 21, 2004
A whistleblower, intimidation by company thugs with threats about ones family, bugging of offices, Richard Scruggs filing lawsuits, and the filing of a counter-suit. A fight against big tobacco, asbestos, or big food? No it is all about a community hospital in rural Georgia. From the Atlanta Journal-Constitution:Hospital challenger feels he's a target:
Charles Rehberg is learning that being an industry whistle-blower has an ugly side.So Rehberg and Bagnato did some investigating of the hospital and were not pleased with the results. They then apparently sent their findings to Scruggs as part of his lawsuit. There was also some unfavorable information about the hospital floating around:
First came the private investigators, who showed up at his medical office parking lot as he was leaving work on the evening of Aug. 9, blocked his pickup and, he says, threatened him and his family.
Then this week came the lawsuit from the hospital system that hired the private investigators. It accuses Rehberg of racketeering and fraud, among other things.
"This sort of thing doesn't usually happen to a CPA," said Rehberg, an accountant who manages Albany Surgical, a general surgery practice.
For the 44-year-old Rehberg, nothing has been usual in the year since he and a prominent doctor at Albany Surgical, John Bagnato, decided to investigate the financial practices and political power of nonprofit hospitals.
The two men spent much of 2003 poring over tax returns, financial statements and databases on nonprofit hospitals, first in Georgia and then nationally. They came to believe that Albany's Phoebe Putney Health System and scores of nonprofit hospital systems throughout the nation were overcharging patients without health insurance and then aggressively seeking payment --- thereby violating their charitable obligation.
The information they gathered --- and delivered to famed Mississippi litigator Richard Scruggs in March --- was the catalyst for a series of lawsuits filed this summer against hospital systems that now total 45.
Langley said he hired former FBI agents, working for an Arizona private investigation firm, to help the hospital determine who in Albany was sending anonymous faxes containing derogatory information about Phoebe Putney. The faxes mentioned, among other things, executive salaries, a Cayman Islands account, and political and business connections.Does Phoebe Putney have its' own "plumber's squad"?
Those faxes, titled "Phoebe Factoids," were sent to local business leaders and politicians....
A lawsuit alleging racketeering and fraud followed two days later, accusing Rehberg and unnamed other defendants of trying to inflict "economic harm" on Phoebe Putney.
The hospital system contends it traced the "Phoebe Factoid" faxes to a phone number at Albany Surgical --- and to a number used by Rehberg. Langley claims the faxes contained falsehoods and innuendo.
Rehberg called the lawsuit against him "absurd." His Atlanta attorney, Robert Mulholland, said the charges were without merit and an attempt by Phoebe Putney to distract attention from its financial practices.
When asked by a reporter whether he had a role in the faxes, Rehberg referred the question to his attorney. Mulholland's response: "We don't discuss the substantive aspects of litigation until we're in court."
There have been other troubling developments. Albany Surgical's president, Dr. Christopher Smith, a longtime critic of Phoebe Putney's administration, said an electronic surveillance device was found within his practice's gray concrete walls. And Rehberg said there was an attempt in February to bug his house.Sounds scary.
It seems to me that these hospitals are being sued because they took steps to avoid running afoul of Medicare regulations which have been interpreted to mean that you could not charge anyone fees below that of Medicare. There was also concern that if hospitals were not aggressive with debt collection they could get into trouble as well. This was cleared up by HHS in a February 2004 memo and hospitals are moving to change their policies.
Some legal scholars have called into question the strength of Scrugg's case.
Some health law attorneys are skeptical that Scruggs' arguments will succeed.Having addressed the facts I would now like to address the possible motives behind this.
"The behaviors they're targeting (billing and collection practices against the uninsured) are atrocious in some circumstances, but they're not illegal," says Gregg Bloche, a law professor of health law at Georgetown University. "The suits will fail."
Nor do they think there is an implied contract between hospitals and the government.
"That's never been recognized in the law," says Stuart Gerson, a partner at Epstein Becker & Green in Washington, D.C., who represents a hospital being sued. "The idea of an individual citizen, a taxpayer, seeking to enforce charitable obligations is, at least, a very novel argument that finds little support."
If any laws are being broken by the common hospital practice of allowing for-profit doctors to use their facilities, or if facilities are improperly steering business to trustees' companies, those arguments should be heard by taxing authorities or federal and state antitrust or anti-kickback regulators, Gerson says.
The lawsuits are renewing debate over the legal and ethical responsibility the nation's non-profits have to provide charity care.
"The IRS has never been really clear about what the grant of tax-exempt status means," says attorney John Reiss of the law firm Saul Ewing in Philadelphia. "It's never been clear that it actually commits you to providing any particular amount of charity care or anything else."
I would like to ask Mr. Rehberg, Dr. Bagnato, and Dr. Smith about the policy of Albany Surgical's concerning payment of bills by uninsured patients. Do they refer individuals to a collection agency after a period of time? How do their debt collection efforts differ from that of Phoebe Putney? Do they turn away uninsured patients from their office? Do they insist on down payments and a payment plan prior to performing elective surgery? If their motivation was to protect the uninsured, the answers would be revealing.
If they were concerned over financial impropriety, why didn't they notify the IRS or the HHS Inspector General? Why ally themselves with Scruggs?
Dr Smith is described as a "longtime critic of Phoebe Putney's administration". Could these actions be in retaliation to some unrelated action on the part of the hospital?
All of this makes for a good soap opera. The fact that it is fairly local makes it even better. This could however evolve into a "cutting off your nose to spite your face" situation. If the hospital takes a severe enough hit, they could be forced to curtail services.
Mr Rehberg must be naive to assume that he wouldn't get some backlash over this. As with many small to medium-sized communities the local hospital is a major employer. And some in the community will not sit back and allow such a major player in town to be attacked without a response.
|
Friday, August 20, 2004
As if time on a dialysis machine wasn't bad enough. From the Atlanta Journal-Constitution: Dialysis, community tie West Nile cases
Two Dougherty County men who came down with West Nile virus a year ago might have been infected during treatment at a local dialysis clinic, the Centers for Disease Control and Prevention warned Thursday.
Then again, the agency said, they might have been infected elsewhere — but it warned that dialysis clinics should take care not to transmit the virus, just in case....
The men, it turned out, were both patients at the same clinic. They had both received dialysis on the same day in late August. In fact, they had both been treated on the same dialysis machine.
There was just one problem. The dialysis clinic, which was examined by investigators from the CDC and the Georgia Division of Public Health, appeared to have done everything perfectly. The investigators could not find a single breach of the infection-control practices that prevent patients from having contact with each other's blood. West Nile, which is primarily passed along by mosquitoes, can be transmitted by blood as well.
|
The good Dr. Rangel has picked up the pet peeve ball and run with it. He tells the story of an orthopedic surgeon who admits a patient to their service, operates on that patient, and during the hospitalization transfers the patient to Dr. Rangel without clearing it. Dr. Rangel has two beefs with this: he wasn't called and the patient was uninsured.
I wholeheartedly agree with Dr. Rangel that the orthopedist owed him a phone call (at least) to discuss the transfer. The actions of the orthopedist in that regard are disreputable to say the least. Dr. Rangel had every right to refuse the transfer.
As for the second issue I wonder, did the orthopedist consult other physicians for medical management of his insured patients or not? If he did then that is a big problem. If Dr. Rangel finds he and his associates are only getting the "self-pay' crowd then that is a problem that must be addressed. Selective referral is a widespread problem with everyone, not just surgeons. One point not made is that surgical procedures fall under what is known as a "global period", usually ninety days. So opposed to a consultant for medical management that can submit a daily visit charge on a postoperative patient, the operating surgeon cannot for "usual" postoperative care.
I have often asked for a medically complicated patient to be admitted to his PCP or the staff medicine service rather than to my service. It works well for me because I don't do a wallet biopsy prior to making the decision and I evaluate the patient in the ED at that time and take them to the OR right away if need be. |
Wednesday, August 18, 2004
As threatened, my travails of last week:
I wanted to buy Doom 3 but my old graphics card was not up to the task. I purchased a GT 6800 overclocked card and installed it last Tuesday. It went smoothly until I wanted to try out a game to see what it looked like. When I inserted the CD ROM into my drive the computer re-booted. That's funny, I thought, until I got the message that no boot device was recognized. When I looked in the BIOS boot sequence all of my drive designations were replaced with "]". I tried for about an hour to get it to work but I was running late and had to go home. I arrived early the next morning to speak with my manufacturer's outsourced technical help. After about 30 minutes while in BIOS he has me type in 'ctrl-alt-b' and 'ctrl-alt-d' and magically it returned to normal. Score an "attaboy" for "Billy".
I was also the resident attending last week. Some tales of the head injured:
Patient #1 was assaulted about 4 weeks ago. He had no insurance and his parents were unwilling to take him home. The tireless efforts of the case managers were able to secure a "scholarship" (charity) bed at a nursing home. His mother's boyfriend put up all kinds of roadblocks to transfer. They wanted to visit the facility. They then became passive-aggressive (not returning calls, visiting after hours, ect) in an attempt to hamper his disposition. What got him out was an ultimatum of nursing home or your home. They chose the nursing home
Patient #2 fell out of a truck. His story began here. He had move from the comatose to flinging his fecal matter around. His family wanted to take him home. Having been burned by the "bounceback" before they had to submit to 48 hours of Dr. Parker's home simulator. The rules:
The nursing staff will check vitals Q shift. They will bring his food and scheduled medicines. You will feed and medicate him. You will bathe him, ambulate him, change him and his bed as needed. If he makes a mess, housekeeping will bring you a pail and bucket for you to clean it up. You may not restrain him. A family member must stay with him at all times. No leaving for eating or smoking. If you require the help of nursing for any of the above reasons the simulation is over and if you take him home you will sign out AMAThey passed with flying colors.
Patient #3 was in a motorcycle collision. As with patient #2 he had a scatalogical temperament. He was ready to go somewhere but the family was playing the "he's not ready game". One day he eloped with the help of his friends. His family brought him back later that day with a drug screen positive for amphetamines,cocaine,THC, and opiates (none on his admission UDS). If we was well enough to go to the local drug corner, he was well enough to be discharged.
To pour salt in the wound I was on call this past weekend. I got a call from the house supervisor, at midnight, that a primary care physician wanted a central line on a patient. The jerk didn't have the decency to roll over in his bed and call me himself. I delivered the old "if he wants the line he has to call me personally" and was undisturbed for the rest of the night.
30 y/o shot center mass by some jackass firing a gun to disperse a fighting crowd. She herself was trying to break up the fight. DOA
Oh yeah, Doom 3: Graphics are excellent, but the gameplay itself is mediocre. The whole "experiment gone wrong" has been done better before with Half-Life. With the unlimited quicksave it is fairly easy. If you had to reach a checkpoint before you saved, such as in XIII, it would make it more of a challenge. Maybe Galen have a better review.
|
Tuesday, August 17, 2004
Sorry about the lack of posting. Busy week last week, but more on that later. An interesting case is that of a 50-ish gentleman who aboout 2 years ago underwent a sigmoid colectomy for malignancy. He was found to have a T3N2, stage III cancer. He did not follow-up for chemotherapy. He showed up in the ED last week with abdominal pain, leukocytosis, and a CT that looks like this:

Line pointing to the hydroureter on the left. Working our way down:

Uh oh. Looks like air where there shouldn't be any. Continuing:

What we have here is a psoas abscess with colonic inflammitory change consistent with diverticulitis. This also seems to be going on at the site of his previous colectomy for cancer. He had no peritoneal signs and had not been on any antibiotics. What to do? Any operative intervention at his point would have committed him to a colostomy, perhaps forever. So I had my radiologist colleauges lend a hand an they placed a CT-guided drain into the abscess. He improved with that and antibiotics. He is afebrile with a normal WBC and tolerating a diet. Follow-up CT:


Diminished size of the abscess, and some po contrast within the contained perforation. His CEA has risen to 98. My plan is to continue to let him "cool off" on antibiotics for a week or so and attempt resection with primary anastamosis. I may still have to divert him with an ileostomy. He will also need a ureteral stent. |
Sunday, August 08, 2004
From MSNBC: Towel found in woman 7 years after surgery
Relatives of a woman whose surgeon left a rolled-up towel inside her chest seven years ago have filed a lawsuit against the clinic where the surgery was performed.
Bonnie Valle often complained about an odd feeling in her chest in the years following a procedure at the Cleveland Clinic, family members said.
"She always said, ;On the left side, it feels like there's something there. It felt like something moved," said her daughter, Jeanne Clark....
When she died in June 2002, a day after her 60th birthday, Valle donated her body to the Northeastern Ohio Universities College of Medicine. During dissection, a faculty member discovered a green surgical cloth the size of a large hand towel behind her left lung.
Wow. It was always interesting when something unusual was found in a cadaver during dissection. But those were usually limited to artificial joints, pacemakers and the like. I'm sure that caused quite a stir in that anatomy lab.
The usual preventative measures don't work in situations like these. Towels are not usually counted and are not radio-opaque, so x-rays won't help.
|
Saturday, August 07, 2004
From The Washington Post: Live! From the OR In Hospital Webcasts, Only the Surgeon Gets in Closer
It wasn't easy for Victor Ganderson, 61, to agree to GERD surgery in June. For four years he had stalled, researching treatment options and talking to his doctors. But it wasn't until the Columbia man watched -- live, via his home computer -- the operation being performed that he decided to go ahead.Apparently the University of Maryland is using the webcasts as a marketing tool for their surgeons. Patients can log on to these sites and watch surgery in action.
Ganderson learned about the "webcast" through his job as a database manager at the University of Maryland Medical Center (UMMC). The surgery was broadcast live on the Internet, from what was billed as the Baltimore hospital's "Operating Room of the Future."
James Gammie, a cardiac surgeon at UMMC, said one patient traveled from Florida for mitral valve repair surgery after her husband found UMMC's Web page describing its minimally invasive surgical technique. "Many [patients] have said they watched the webcast," Gammie said in a telephone interview. "So I find that probably 50 to 60 percent of people who come to us now . . . are much more prepared." Gammie provided commentary during the mitral valve operation while another doctor performed the surgery.As usual there is someone to rain on the parade:
Some consumer health advocates question the webcasts' value to consumers. Arthur Levin, director of the nonprofit Center for Medical Consumers in New York, said he thinks a surgical webcast serves more as a public relations tool for hospitals than as education for consumers.What would happen if something went wrong?
"The important things that patients need to know about surgery are: What are the risks? What are the alternatives? That's the kind of information people need. They don't need to see someone else's stomach open," Levin said.
Dr. X: We are dissecting around Mrs. Smith's esophagus now with our retractor. This will allow us to get the fundic wrap around the back.
Dr. Y: Hey! Does that look like an NG tube to you?
Dr. X: Damn it! We've put a hole in the esopha...
Then as Mrs. Smith's family is calling the John Edwards law firm you see on your screen:

Oops!!!
What if something unexpected occurs?
Dr. X: We have just placed all of our ports into Mr. Jones' abdomen and will now take a look around..So now everyone on the internet knows about Mr. Jones and his liver tumor before Mr. Jones and his family do. Such problems could be avoided by "tape delay" of procedures, but that would eliminate the "live chat" feature which appeals to the marketers.
Dr. Y: Hey! Does that look like a tumor on the liver to you?
Dr. X: Yes it does. Let's send some for a frozen section...
Live broadcasts allow viewers not only to watch but to e-mail in questions, some of which are answered by an operating room narrator while surgery continues.....Yes, the faculty, whose job also consists of training the surgeons of tomorrow. How many residents get "face time" with the webcasts? Organized medicine has spoken on this before:
A surgical webcast "allows us to demonstrate our expertise, both the physician expertise as well as the expertise of our facility," said Dave Brond, UMMC's vice president of marketing and planning. "It also wasn't a traditionally used part of our marketing toolbox. . . . This is a way of funneling more people into our Web site who are searching for health care information online."
The Society of Thoracic Surgeons issued guidelines in 1998 advising against live broadcasts of thoracic surgical procedures to the general public.The patients watching the webcasts could get a biased view of surgery:
"The Society believes a possibility exists wherein participating surgeons might fail to follow proper medical procedures or might be distracted because of the media and, thereby, deprive the patient of the highest quality care," the guidelines say.
Hospitals often choose to broadcast minimally invasive procedures, Aitchison said, because these transmissions show off new technology while featuring procedures that reduce patient discomfort and recovery timeNot all procedures planned as minimally invasive end up that way. Even in the hands of experts sometimes you have to convert to an open operation.
Privacy may be affected. I'm sure the patient who is the star of the show signs all kinds of waivers before the procedure, but there are situations where sensitive medical information about others may be discussed (answering the pager for example) which may not be covered.
Such broadcasts, live or otherwise, have been used in surgical education for years. Walk through the display floor at an ACS meeting and Ethicon, U.S. Surgical, and many others will have scheduled "live procedure broadcasts" as they try to get you to buy their stuff. The ACS itself was video clinics where surgeons submit material for review and broadcast (I have "starred" in one of those). But the target audience for those are aware of the god, bad, and ugly of surgical procedures. The general public may not be as "nuanced". Their expectations may be raised, possibly to an unreasonable level, by this sort of thing.
|
Friday, August 06, 2004
Looks like the folks on the other side of the blood-brain barrier have a new toy. From CBS: Goggles Give Docs All-Seeing Power:
Patients and their crises come and go non-stop at Vanderbilt University Medical Center.The goggles also have the ability to access the surgical schedule and the hospital computer.
So anesthesiologist Paul St. Jacques somehow has to keep up with four operating rooms at once -- good thing he can see through walls.
Anesthesiologists here routinely are responsible for four operating rooms at once.
Only now, as CBS News Correspondent Mark Strassmann reports, St. Jacques literally can keep an eye on all of them at the same time.
Attached to his goggles is a tiny screen, about the size of a fingernail, and there's a video-panel from each of the four on-going surgeries, real-time images of his patients and their vital signs.
No comment on how the system has improved their crossword puzzle skills.
|
Thursday, August 05, 2004
From the Boston Globe: Panel urges standards for obesity surgery
Responding to a sixfold jump in the number of patients undergoing obesity surgery, a state public health panel yesterday recommended that Massachusetts hospitals and doctors adopt strict standards to reduce deaths and complications.The report from the panel, which may be found here is quite detailed. Over 100 recommendations are put forth, from insuring that hospitals offering bariatirc surgery have special operating tables, longer instruments, wider wheelchairs, and so forth. There are also recommendations about both hospital and surgical volume:
The report includes recommendations that hospitals and surgeons perform a high number of surgeries in order to stay in practice, which ultimately could force some smaller programs at community hospitals to close. Based on their review of medical studies, panel members said hospitals that do more than 100 surgeries a year, and surgeons who do 50 to 100 cases a year, have lower complication rates.
One guideline recommends surgery only at hospitals that perform 100 or more cases annually. Only 14 of the state's 24 hospitals that do obesity surgery perform that many, said Dr. George Blackburn, vice chairman of the panel and a physician at Beth Israel Deaconess Medical Center. The panel also recommended that hospitals adopt strict standards for doctors before allowing them to perform obesity surgery.So over half of the hospitals in Massachusetts providing bariatric surgery do not meet the goals set forth in the report. Lets look at the details of the suggested volume requirements (page 17 of the PDF file):
For traditional weight-loss surgery, during which doctors make a long incision, hospitals should have an experienced surgeon monitor a new surgeon for 10 cases. The hospital should then review the next 15 cases of the new surgeon, to make sure standards are met, before granting full privileges to the surgeon.
So before a surgeon could even perform the procedure unsupervised they would have to undergo training, perform 10 proctored open procedures and 25 proctored laparoscopic procedures. Some allowance would have to be provided for surgeons who performed bariatric surgery in residency. It seems to me that it would be hard to find ten patients willing to undergo open bariatric surgery nowadays with the popularity of laparoscopic surgery. Continuing:1. Establishment of Provisional Privileges (open WLS procedures)
• Completion of the (ASBS) American Society for Bariatric Surgeons essentials courses or equivalent
• Successful completion of 10 open cases proctored by a surgeon with full privileges for open WLS.
1a. Establishment of Provisional Privileges (laparoscopic WLS procedures other than
LAGB)
• Meets requirements for provisional open privileges
• Successful completion of 25 laparoscopic cases proctored by a surgeon with full
privileges for laparoscopic WLS (Category B).
2. Establishment of Full Privileges (open or laparoscopic WLS procedures)So even after the 35 cases required above, an additional fifteen would have to be reviewed. The surgeon would then be required to perform at least fifty a year.
• Review of first 15 independently performed cases by a committee that includes the chief of surgery at the surgeon’s institution and an experienced (>100 cases) weight loss surgeon; this committee may also include members of the institution’s Quality Assurance and Credentialing programs
• No substantial deviation in risk-adjusted outcomes from accepted norms and
benchmarks.
2a. Recredentialing of Full Privileges (open or laparoscopic WLS procedures)
• Maintenance of board certification or board eligibility. Credentialed gastrointestinal surgeons who are active staff member with full admitting privilege at facility obtaining bariatric privilege are eligible
• 100 primary or revisional WLS procedures within the previous 2 years (Categories B and D)
• Presence of a second weight loss surgeon on staff with either full or provisional privileges within the same program
A very good effort to assure quality control concerning a very risky procedure. It will be interesting to see how they work out, especially the volume requirements. Some "grandfathering" of these regulations are likely. This could still dissuade a surgeon from going off to a weekend course and proclaiming themselves a bariatric surgeon. The hospitals that are not currently meeting those goals will be very reluctant to let potentially very lucrative bariatric surgery business leave. Another problem is that if all of the procedures are shunted to a few centers in the state the desire to take care of the complications by other surgeons not working at the "Bariatric center of Excellence" will fall, for reasons explained in this post. Stay tuned.
|
Wednesday, August 04, 2004
From Scrapple Face Kerry Hires Edwards to Sue DNC Over 'Bounce'
(2004-08-03) -- Democrat presidential candidate John Forbes Kerry today announced that he has retained attorney, and running mate, John Edwards to file suit against the Democrat National Committee (DNC) over injuries related to an alleged "post-convention bounce."
"We had received certain assurances from top DNC officials that this celebration of my client's nomination would result in a 10-15 point bounce in the presidential preference polls," said Mr. Edwards during a news conference on the steps of a Boston courthouse. "Bounce implies vigorous upward movement. But my client's current polling numbers look more like a 'bump' or even a 'dip'."
Mr. Edwards, who like his client is also a U.S. Senator, brought many of the gathered journalists to tears with his dramatic description of the plight of Mr. Kerry's popularity.
"I can hear John Kerry's popularity calling out to you from somewhere in the darkness," said Mr. Edwards. "A couple of weeks ago his popularity said, 'I'm fine." Just before the convention it said, 'I'm having a little bit of trouble but I'm doing okay.' During the convention speech, it said 'I'm having problems.' And after the convention John's popularity said, 'I need help.' But help was not on the way."
What is the political equivalent of a cesarean section?
Har har....
|
Just when I thought I could get away from West Virginia malpractice posts this gets served up in the Charleston Daily Mail:Award-winning physician faces insurance problems
Dr. James Blume was the first West Virginian and the first osteopathic physician in the United States to win the National Country Doctor of the Year award, in 2002.Apparently Dr. Blume has fallen through the cracks of liability insurance despite the promise the physicians mutual once held:
Gov. Bob Wise has named the rural Summers County physician a Distinguished West Virginian.
And, board certified in family medicine, Blume last year received the Off-Campus Teaching Award from the West Virginia School of Osteopathic Medicine.
Despite his accolades, Blume can't get medical malpractice insurance from the new West Virginia Physicians' Mutual Company formed by legislators to help state doctors find coverage.
Blume said the new physicians-owned company isn't doing what legislators said it would.Remember, this is an insurance company that obtained its operating capital from an $1000 assessment from all licensed physicians in West Virginia. The contributors did not receive any shares in the mutual company for their $1000. On the other hand, by law, a physician who did not pay the assessment was subjected to suspension of their license. If they wanted to regain their license they were required to pay the assessment and an additional $250 fine. While the money may or may not be significant, the fact that your license was suspended is. You would then be subject to the dreaded "please provide additional information" instructions on any number of forms.
"Physicians in particular and citizens of the state in general have been sorely misled, as demonstrated by the recent turn of events in my career," he wrote in an open letter dated Monday.
The mutual's CEO, David Rader, said the company's underwriting criteria have been approved by the state Insurance Commission. Because of a capacity problem, it's not possible to accept all physicians who apply for coverage, he said.
For instance, about 1,400 physicians transferred from the state Board of Risk and Insurance Management to the mutual July 1. Another 100 physicians have applied and about half of those have been accepted.
"There have been a few declinations, 15 percent to 20 percent," Rader said
My philosophy is that businesses should be free, within the law, to associate with whomever they please. But this physician was, in effect, extorted by the State of West Virginia and the West Virginia Board of Medicine, to benefit this company who won't even provide him insurance. If he was a menace to patients that is one thing, but a physician with three suits that he won certainly does not fit that description.
The mutual insurance company isn't living up to expectations in this case:
In his July 1 address in kicking off the mutual, (West Virginia Governor Bob ) Wise said the state must "guarantee . . . that every West Virginia doctor has access to reasonably priced medical malpractice insurance."
I wonder if Dr. Blume will get his $1000 back?
|
Tuesday, August 03, 2004
Galen relates a story of a patient trolling for his phone and pager number. Much to his credit he held firm and didn't give it out. My paranoia extends so far that I have an unlisted number and my number does not appear on caller ID screens. For those who have "no ID" blocks on their phones I call my answering service and have them make the call for me. I do the same when I return calls from my cellphone. I've heard stories of physicians forced to change their phone numbers because patients would write their numbers down from caller ID. |
20-ish y/o restrained driver in SVMVC. +LOC with complaints of abdominal pain and facial pain. Hemodynamics are stable. Otherwise healthy. Undergoes CT of abdomen:
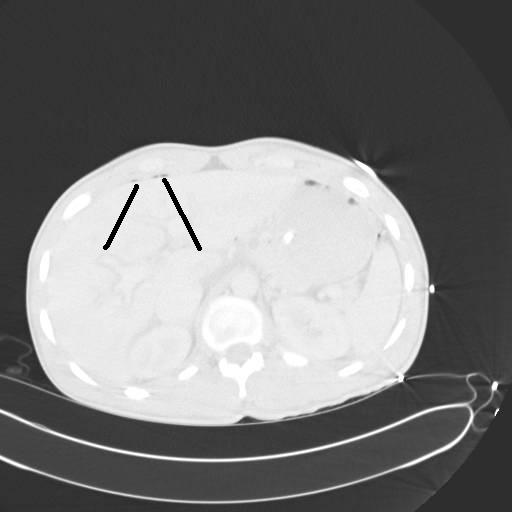
The black lines point to two small areas of free air. He is also found to have a nasal bone fracture but no other acute findings on CT. He is taken to the OR for an exp lap with findings of a jejunal tear which is repaired without difficulty. Two days later he complains of inability to move his right leg. Sensation to coarse touch and proprioception is intact. He has diminished pulses in that foot. Some pain on passive range of motion but no bony crepitus. A noninvasive vascular study is ordered and reveals an ankle-brachial index of 0.9 on the left and 0.6 on the right. An angiogram is ordered:

This is a view of his superficial femoral artery. Looks good but you can see some problems beginning distally.

What you see here is occlusion of his popliteal artery above the knee with reconstitution of the below-knee popliteal and filling of the trifurcation. Notice the size of the collaterals.

Unfortunately he appears to only have one-vessel runoff to his foot. Our diagnosis at this time was popliteal artery injury, likely due to a knee dislocation which had spontaneously reduced. We were not totally convinced due to his lack of joint instability. The initial plan was to attempt a stent-graft across the area of injury. (By this time my vascular surgeon partner was along for the ride.) We were able to get a wire and catheter through a collateral but not into the main artery. After further angiography we determined that what the patient had was not an acute injury but popliteal artery entrapment syndrome. The patient then underwent a popliteal to popliteal bypass with reversed saphenous vein. Upon further questioning he did state he had experienced worsening leg pain over the past few weeks but had attributed it to "soreness". This patient fits the profile in the article very well. Young, active and otherwise healthy. It was fortunate the condition was discovered while his foot was still viable, since embolization can be a complication. The size of the collateral vessels on his angiogram provide an indication of the long-standing nature of this problem when compared to a more acute change.

Where the vessels are smaller. He is doing well and has regained motor function in his lower extremity |
Apparently I was not alone. From American Medical News: $1,000 licensing fee hard to swallow
Some physicians would rather give up their medical licenses than pay $1,000.So, based on the above numbers, 5.5 percent of West Virginia's allopathic physicians and 7.1 percent of osteopaths chose not to renew their license. Certainly almost all of those who surrendered their licenses were out-of-state such as myself, or retired. What was not mentioned was the fact the WVBOM allowed the option of going to an "inactive" license. This cost $100 (instead of $300 for a full license) and you did not have to pay the assessment.
More than 350 doctors told West Virginia's medical boards they would not renew their licenses after July 1, the day the state began assessing a new $1,000 fee per license to help fund a physicians mutual insurance company. But state officials said the doctors' decision not to pay has not greatly altered the number of doctors practicing in the state.
The West Virginia Board of Medicine said 309 MDs of the 5,575 with licenses said they did not want to renew. "Most of the people that chose to lapse their license were probably out of state," said Ronald D. Walton, the board's executive director. The licenses of another 70 MDs were suspended by the board, Walton said. As of July 22, 14 of those were reinstated after the physicians paid the $1,000 fee and $250 late payment.
Of 61 DOs who decided not to renew, "Most of those were out-of-state physicians who were not practicing in West Virginia anyway," said Cheryl Schreiber, executive director of the West Virginia Board of Osteopathy, which covers 850 doctors. "Of those, 25 of them told us the reason they're not renewing was because of the assessment."
The board also sent notices to 45 doctors, telling them their licenses were suspended as a result of nonrenewal. Schreiber said some have since paid the $1,000 assessment and a $250 late fee.
The assessment was started July 1 to help fund a physicians mutual insurance company, which was created by the state Legislature last year due to the medical liability crisis in the state. The company covers about 1,400 physicians. Some physicians are exempt from paying the assessment, including medical school faculty and physicians in the military.
The West Virginia State Medical Assn. was against the assessment, said Evan Jenkins, association executive director. But, he said, "The physicians mutual is important for addressing the crisis of insurance availability."
Jenkins said physicians are trying to adjust to the fee. "The reactions are mixed. Nobody likes to be told they have to contribute $1,000."
The economic impact on the board may be significant. With the renewal fee of $300, the board has lost $92,700 already. If the 56 with currently suspended licenses do not renew, the loss grows to $109,500. The osteopathic board fees run $200 so their loss of revenue is $12,200. Of the 45 who were suspended, "some" have paid, but the loss could rise as well.
Such is the cost of doing business.
|
Monday, August 02, 2004
From MSNBC:Young doctors reportedly working fewer hours
Doctors fresh out of medical school are working fewer hours compared to their predecessors, thanks to new rules that went into effect a year ago curbing duty time. But growing pains abound. Some medical students and experienced doctors are getting stuck with more work and hospitals are spending millions of dollars overhauling work schedules.So far compliance has been fairly good:
Most residency programs are in compliance with the new standards, according to the accreditation council. Since last July, it reviewed 2,019 programs — or about a quarter of total programs — and cited 5 percent for duty-hour violations. Nearly half of the offenses were for breaking the 80-hour week limit.The AMSA, however thinks that the number is under-reported. Now for an update from the "unintended consequences" department:
The accreditation council also allowed 75 surgical programs to extend resident work hours to 88 hours a week. So far, 53 doctors have filed complaints about work-hour breaches. Eleven cases were dismissed for lack of evidence.
The association also found that medical students — those not ready for residency — are working more. Early results from a survey of 488 students found that half reported finishing clerical work for residents and a quarter said they completed clinical duties.What sort of "clinical duties" are they talking about? Dressing changes? Pulling drains? I did that sort of stuff as a student in "the bad old days".
Well it could be worse, we could live in Europe.
UPDATE: The Resident Wife has more here. |
![]()





